Executive Summary
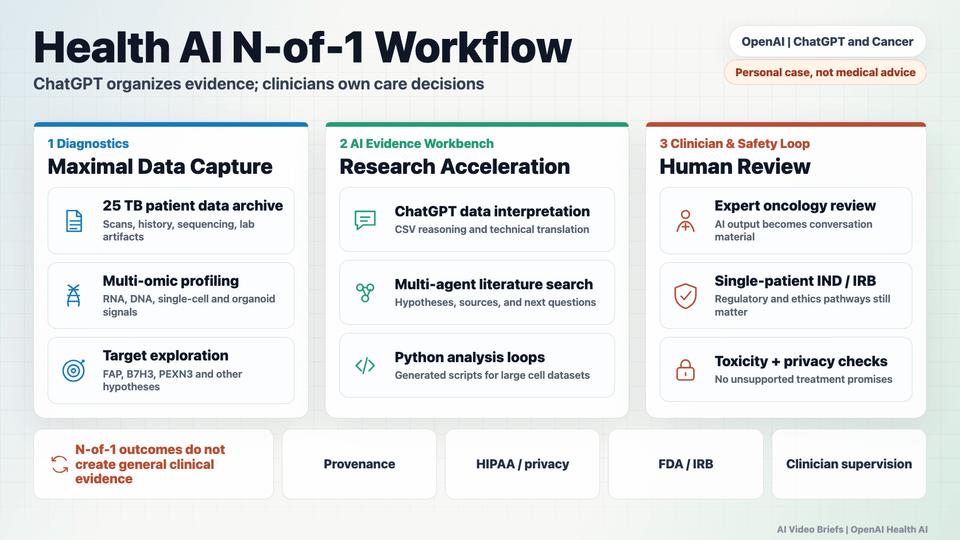
The video follows a technology founder facing recurrent osteosarcoma, a rare bone cancer with a difficult prognosis after recurrence. With standard options limited, the patient team adopted a "founder mode" approach: gather as much diagnostic data as possible, open-source 25 terabytes of biomedical material, and use that evidence to discuss individualized experimental options with medical experts.
AI is presented as an evidence-organization layer, not as the treating physician. ChatGPT and a custom multi-agent harness were used to inspect raw CSVs, search literature, generate Python analysis scripts, triage potential targets, and translate dense bioinformatics into questions that specialists could review. The video highlights examples including B7H3, FAP, and PEXN3 (panexan 3).
The builder lesson is powerful but narrow. This is an exceptional single-patient story with major resources, clinical supervision, regulatory work, and experimental interventions. The page should not imply that ChatGPT treats cancer or that the same pathway is broadly available. The durable product questions are provenance, privacy, verification, toxicology, and clinician-in-the-loop design.
Key Takeaways
- The video is best read as an N-of-1 case study in AI-assisted medical research, not as general cancer treatment guidance.
- The patient team compiled and publicly shared roughly 25 terabytes of biomedical data, including sequencing, organoid, imaging, and clinical materials.
- ChatGPT was used to help inspect raw bulk RNA count tables and surface candidate targets for expert review.
- The video reports that FAP expression helped the team identify an experimental radioligand option in Germany, with a reported 60% necrosis result.
- A custom multi-agent harness coordinated literature search, hypothesis generation, and Python code execution across large single-cell datasets.
- The speakers describe one AI analysis workflow as costing roughly $20 in API usage and taking about 30 minutes of deep reasoning time.
- Sid also argues that raw inputs are becoming more accessible, citing roughly $50 bulk RNA sequencing and whole-genome sequencing starting around $500.
- The case included parallel exploration of highly personalized interventions, including a custom mRNA neoantigen vaccine described as moving from design to injection within about six months.
- A B7H3-targeted scan in Beijing reportedly revealed high liver expression, which shifted the team toward a proposed AND-gate CAR-T design requiring both B7H3 and FAP activation.
- The PEXN3 example illustrates how AI-assisted search can push attention toward understudied targets, but the therapeutic relevance still needs independent validation.
- The IRB and single-patient IND discussion is as important as the AI story: administrative, ethical, and regulatory bottlenecks shape what can actually happen.
Builder Implications
- Build health AI around provenance: every target, source, script, and recommendation needs a traceable evidence trail.
- Separate AI evidence workbench behavior from clinical decision-making; the product should prepare expert review, not replace it.
- Design ingestion for messy medical reality: raw CSVs, imaging, long records, lab artifacts, and specialty vocabulary all need structure.
- Use multi-agent workflows only with strong auditing, because autonomous literature search and generated code can produce plausible errors.
- Make privacy, consent, data retention, and regulatory context first-class UX and infrastructure requirements.
Things to Verify
- Whether generated Python scripts and biological claims are independently checked before they influence patient-care conversations.
- The clinical safety, drug-drug interaction, cross-toxicity, and organ-toxicity profile of any experimental or parallel treatment combination.
- The exact FDA single-patient IND, IRB, and international regulatory constraints for a specific intervention.
- The biological fidelity, leakage risk, and off-target behavior of proposed logic-gated CAR-T constructs.
- HIPAA, consent, and privacy boundaries when moving raw health records and multi-omic files through commercial AI tools.
- Whether targets such as PEXN3 (panexan 3) show reliable expression, binding, and therapeutic relevance beyond this single case.
- Which parts of the reported outcome came from surgery, radioligand therapy, vaccines, AI-discovered targets, or other interventions.